Corpus: Facial nerve


from Latin: facies - face
Synonyms: intermediofacial nerve, nerve VII, 7th cranial nerve
1. Definition
The facial nerve is the 7th cranial nerve. It carries special visceromotor fibers that innervate the facial muscles. It also receives general visceromotor, special viscerosensory and general somatosensory fibers via the intermediate nerve.
To emphasise the composite nature of the nerve more clearly, it is also referred to as the intermediofacial nerve.
2. Embryology
The facial nerve is counted among the branchial arch nerves and develops from the nerve of the 2nd branchial arch. It therefore innervates all muscles that have formed from the muscle anlage of this gill arch, especially visceromotor muscles.
3. Course
The fibres from the run in an arc medially around the abducens nucleus (nucleus nervi abducentis) and form the inner facialis knee. They then meet the fibers of the other two nuclei, which join to form the intermediate nerve. Both parts of the nerve leave the brain separately in the area of the cerebellopontine angle and then quickly unite to form the common facial nerve. The newly formed nerve travels via the internal acoustic pore into the internal acoustic meatus of the petrous bone, at the fundus of which it enters the canalis nervi facialis.
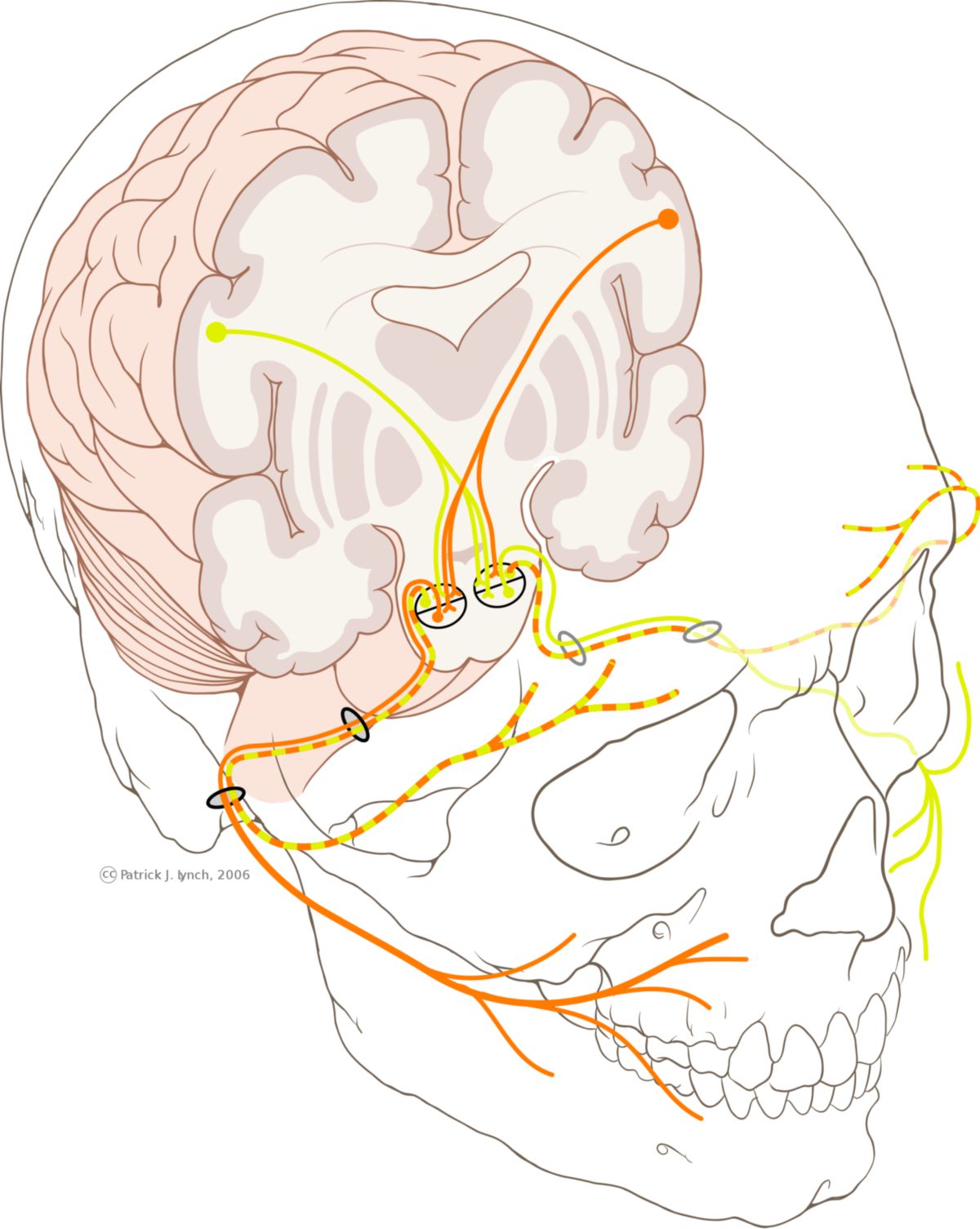
In the region of the petrous bone, the facial nerve forms the geniculate ganglion, where the perikarya of the afferent fibres are located. These fibers continue to the nucleus of the solitary tract. Due to a bent course of the nerve canal, the nerve forms a second, outer "knee", known as the geniculum nervi facialis.
3.1. Branches
Still in the petrous bone, the facial nerve gives off three branches: the greater petrosal nerve, which contains parasympathetic fibers for the innervation of the lacrimal gland; the stapedial nerve for the supply of the stapedius muscle; and the chorda tympani.
After exiting the petrous bone through the stylomastoid foramen, additional branches arise: the posterior auricular nerve and the stylohyoid and digastric rami, which run to the musculature of the neck.
The facial nerve continues into the parotid gland, where it forms a fine nerve plexus called the parotid plexus. It can be divided into two main branches, the upper pars temporofacialis and the lower pars cervicofacialis, both of which then quickly subdivide into finer branches.
3.2. Parotid plexus
The parotid plexus, also known as the intraparotid plexus, lies between the superficial and deep parts of the parotid gland and primarily innervates the facial muscles. The following branches emerge from it:
- Temporal branches: They run over the zygomatic arch into the temporal region and innervate the orbicularis oculi muscle and the corrugator supercilii muscle.
- Zygomatic branches: They cross the zygomatic arch to the lateral corner of the eye and supply the major and minor zygomatic muscles, as well as parts of the orbicularis oculi muscle.
- Buccal branches: Running alongside the parotid duct and the transverse facial artery, these branches extend frontally into the buccal region below the orbit and into the perioral region. They supply the buccinator muscle and the orbicularis oris muscle, among others.
- Mandibular marginal branch: This branch runs below the depressor anguli oris muscle and the platysma, innervating the mimic muscles of the lower lip and chin.
- Cervical branch: Running below the platysma to the neck, this branch forms an anastomosis with the transverse cervical nerve, formerly known as the superficial ansa cervicalis. It innervates the platysma and the skin above it.
4. Fibre qualities and innervation
Like the vagus nerve and the glossopharyngeal nerve, the facial nerve carries motor, sensory, sensitive and parasympathetic fibres. It is formed by around 10,000 nerve cells, of which around 7,000 send out myelinated motor fibres. The other 3,000 cells belong to the intermediate nerve and have parasympathetic, sensory and sensitive non-myelinated fibres.
4.1. Motor parts
The special visceromotor parts of the facial nerve from the primarily innervate the facial muscles and the posterior parts of the suprahyoid muscles, i.e. the stylohyoid muscle and the posterior head of the digastric muscle. There are also fibres that run to the stapedius muscle and are responsible for the fine regulation of hearing.
4.2. Sensory parts
The special viscerosensory fibres of the nerve run with the chorda tympani via the intermediate portion into the nucleus of the solitary tract and ensure the innervation of the taste buds in the area of the lingual papillae in the anterior two-thirds of the tongue. The perikarya of the pseudounipolar neurones are located in the geniculate ganglion, which corresponds to a spinal ganglion.
The general somatosensory fibres of the facial nerve run to the skin of the external acoustic meatus and the tympanic membrane; from there they transmit pain and touch stimuli as well as temperature sensations (caloric nystagmus).
4.3. Parasympathetic parts
The facial nerve receives parasympathetic or general visceromotor nerve fibres from the superior salivatory nucleus via the intermediate nerve, which run with the chorda tympani to the oral cavity and ensure the innervation of the oral salivary glands. In addition, parasympathetic parts of the facial nerve run to the lacrimal gland as the greater petrosal nerve and innervate it.
5. Nuclei
The nuclei of the facial nerve are located in the lower part of the pons and in the medulla oblongata. They include:
- Nucleus of facial nerve (Nucleus nervi facialis)
- Superior salivary nucleus (Nucleus salivatorius superior)
- Nucleus of solitary tract (Nucleus tractus solitarii)
The nucleus of the solitary tract also receives fibres from the glossopharyngeal nerve and the vagus nerve.
6. Clinical significance
The facial nerve can be damaged in a number of diseases; the consequences are usually signs of paralysis (facial nerve paresis).
Such paralysis can either occur in the peripheral area of the nerve and be caused by infectious diseases (Lyme disease, zoster oticus), mechanical damage (petrous bone fractures) or tumors, or be due to central damage. Other important causes are cerebral haemorrhages, cerebral infarctions or space-occupying lesions, particularly in the cerebellopontine angle (cerebellopontine angle syndrome).